My Blood Clot Story
When You Run Out of Mondays
A personal account of two pulmonary emboli, one awkward word, and the curiosity that changed everything.
For months, I felt off. Fatigued, flu-like, and winded climbing stairs. Groceries carried from the car felt heavier than they should have been. I dismissed it with a familiar promise: “Come Monday, I’ll eat better. I’ll move more.”
In the early morning hours of May 2016, my body stopped trying to grab my attention with subtlety. I woke from a sound sleep with a heart pounding like it was trying to escape my chest. I told myself it was anxiety. I’d lost both of my parents within three years of each other and grief has a way of living in the body long after the funeral.
I got out of bed bargaining with my brain. “We can walk this off.” Each step made breathing harder, the heart pounding louder. I slowly walked to my husband’s side of the bed and whispered: “We need to go to the ER. I think I’m having a heart attack.”
Don’t bargain with your body.
Listen to it.
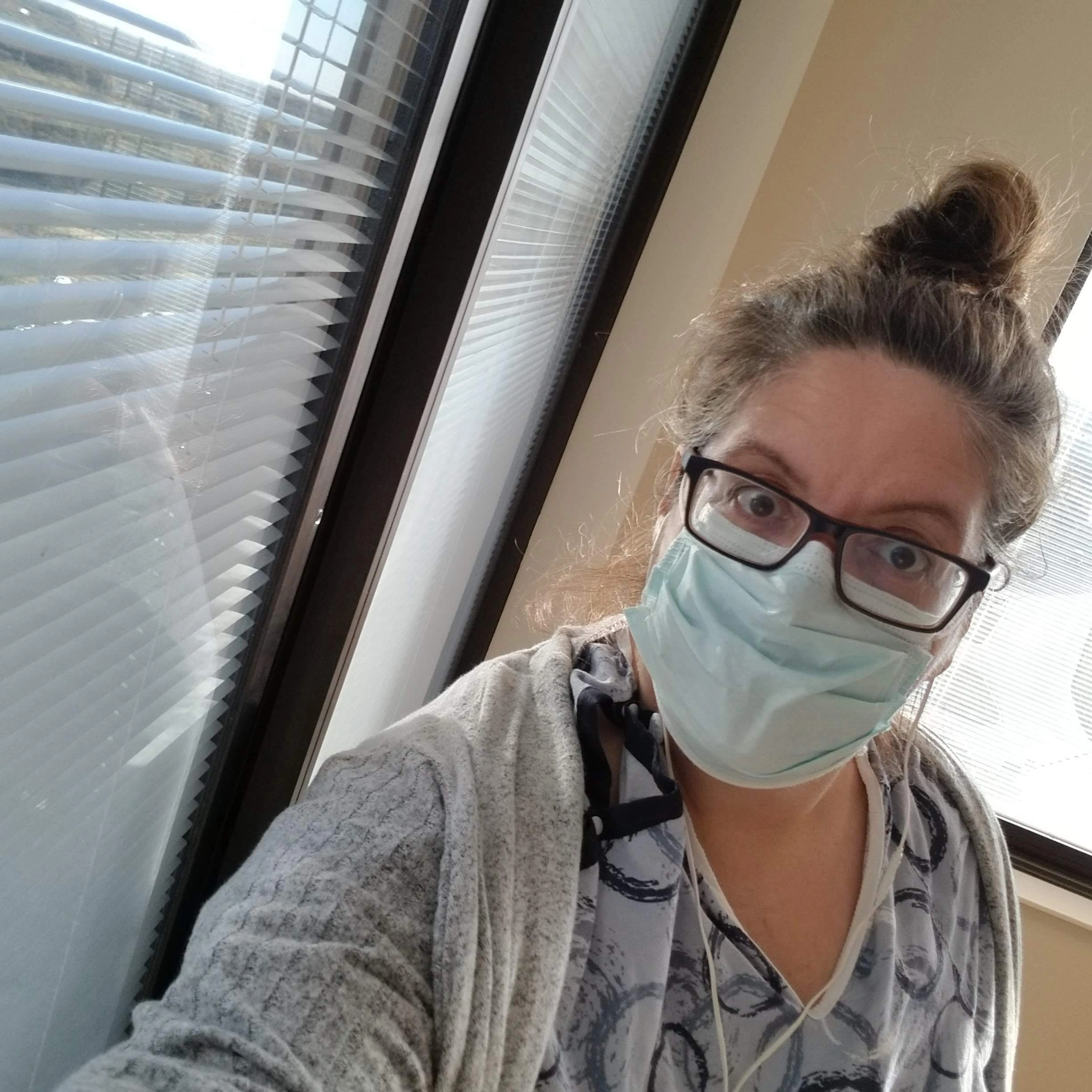
I arrived at the ER where chaos quickly became controlled, coordinated critical care. Lines and leads attached. IV bags hung. Blood drawn. Questions asked and scans ordered.
Thirty-two minutes later, the ER physician presented everything that had been gathered. “Ms. Conley, the good news is you are not having a heart attack. You do have a large blood clot in the main artery of your lung — a saddle pulmonary embolism.
You’re going to spend a little time with us and we’re going to take good care of you.”
I was admitted to the ICU, where I met my vascular surgeon who explained the options, including a newer intervention called the EKOS Endovascular System. A minimally invasive procedure that ran a catheter from the jugular vein in my neck to my pulmonary artery, combining ultrasound energy with clot-busting drugs to break up the clot and relieve the load on my heart.
I was released from the hospital three days later to navigate a new chapter, surviving an almost fatal blood clot.



An awkward label that never fully fit.
For a year, I followed instructions: Warfarin monitoring, genetic testing, and a review of every standard risk factor. There was no recent travel, no surgery, and no estrogen. Despite having a family history, my bloodwork showed no inherited thrombophilia.
Eventually, my pulmonary embolism was labeled “unprovoked.”
Genetic testing doesn’t capture everything. You can have a family-specific clotting factor that standard panels miss. Clots and genetics are complicated — and there is still a great deal the science doesn’t know.
Have you heard the saying “genetics load the gun, but your lifestyle pulls the trigger”? Present were: obesity, sedentary habits, chronic stress, and poor sleep. I share this not from a place of judgment but so you know. These are recognized contributors to cardiovascular and venous thromboembolism risk, not sudden triggers, but the kind of conditions that shape vascular health over years.
Without a plan to address them, those conditions followed me. Four years later I was back in the same hospital with a second unprovoked pulmonary embolism.
My lowest point. And the clue that changed everything.
A week in the ICU, then the cardiac unit. My lowest point, physically and mentally. I lay there racking my brain trying to figure out how I had gotten here again. I thought I had done all the things right.
Then I found the clue that changed everything.
Two months before my second PE, a peer-reviewed study had been published in an American Heart Association journal: Mitigation of Venous Thromboembolism Risk through Favorable Lifestyle — the ARIC Study. Reading it was like someone had opened a jigsaw puzzle and dumped it out in front of me. I couldn’t see the final picture yet. But I finally had pieces to work with. It wasn’t a study about recurrence. It was a study about risk, and it told me that lifestyle had a seat at the table that nobody had offered me.
I’m not certain my lifestyle caused my first clot. But I stopped being certain it didn’t. That uncertainty was the beginning of a question I couldn’t stop asking:
“Why isn’t lifestyle part of the conversation after a clot?”
That question became this platform.


Medicine is powerful.Val Conley — Blood Clot Survivor & Founder, Speaking of Blood Clots
It is not omniscient.
Stopping the wait for Mondays.
Today, I’m in a long-term relationship with apixaban, and anticoagulation is part of my life. So is chronic venous insufficiency, a quiet reminder that clots leave lasting marks. But something changed after the second event: I stopped waiting for Mondays.
I began building habits, slowly, imperfectly, consistently. Movement became non-negotiable, sleep became protected, and nutrition became intentional rather than punishment. Over time, my relationship with my body shifted from reactive to proactive. From criticism to gratitude for what it has, and continues to, carry me through.

Today — still asking questions, still building the conversation.
Health literacy became non-negotiable, not because I’m interested in replacing medicine, but because I’m determined to participate in it fully and so no other woman waits until Monday.
The research exists. The framework is here.
Start with one habit.
Four pillars. One foundation. Find yours.
Every piece of content on this platform lives inside one of these four areas. Start with the one that’s calling you.

Not medical advice. Val Conley is a VTE lifestyle educator and survivor, not a clinician. This site provides general information only — not a substitute for professional medical advice, diagnosis, or treatment. If you believe you are experiencing a medical emergency, call 911. Read full disclaimer →